Stages, grades, and risk levels
NMIBC is categorized by stages, grades, and risk levels. These different categories help your doctor determine the best treatment strategies.
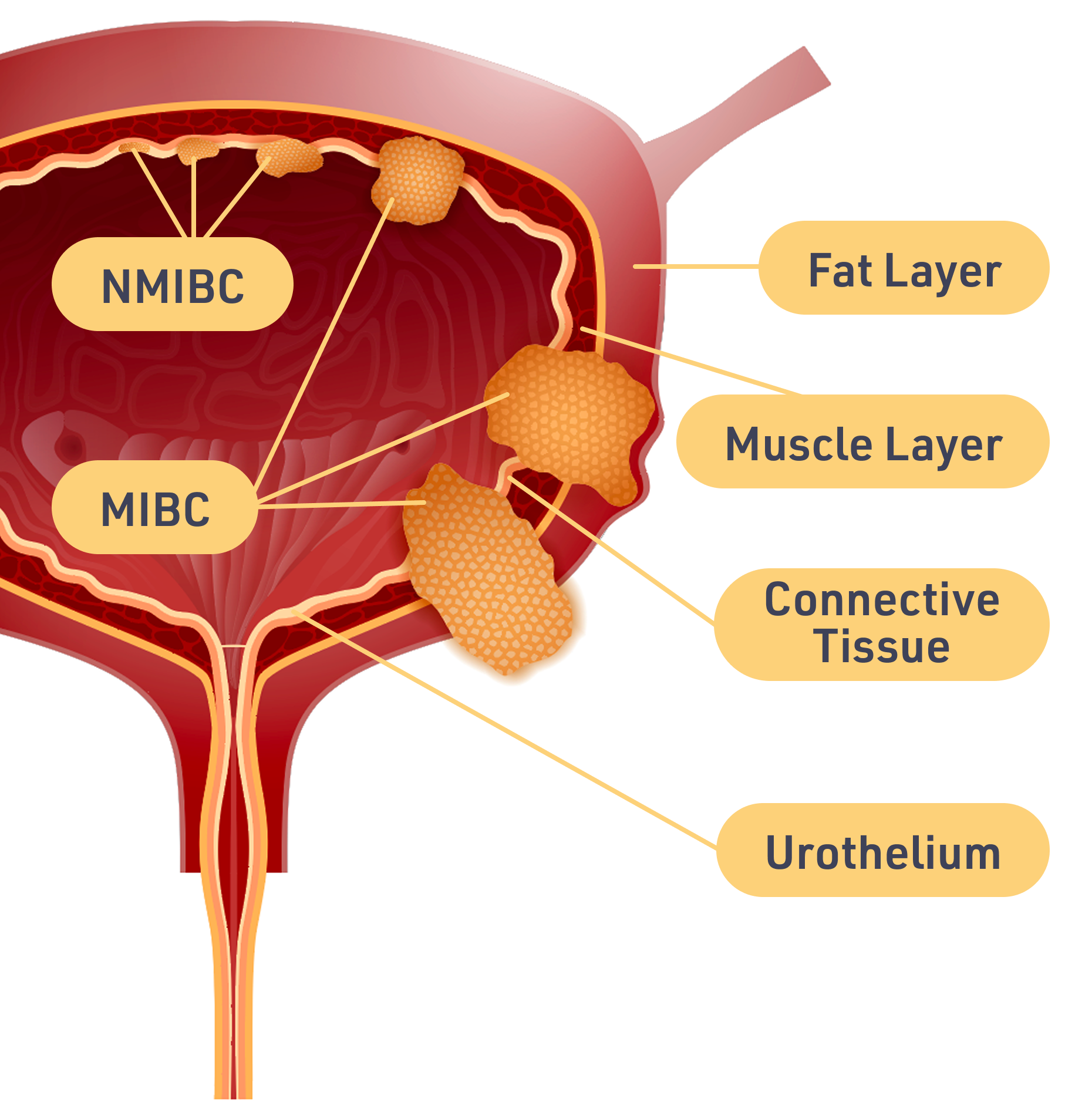
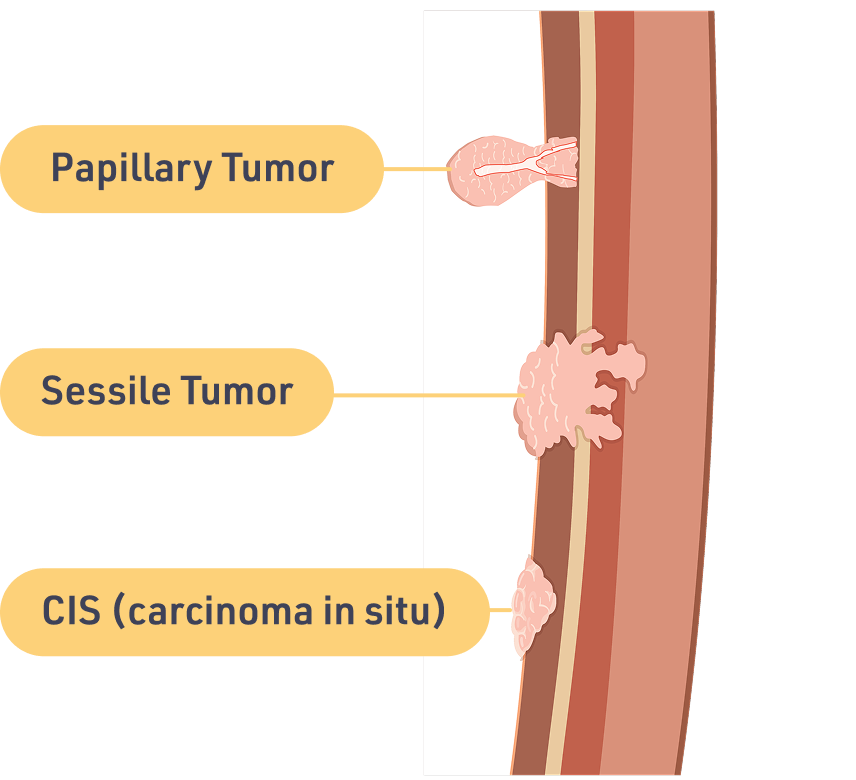
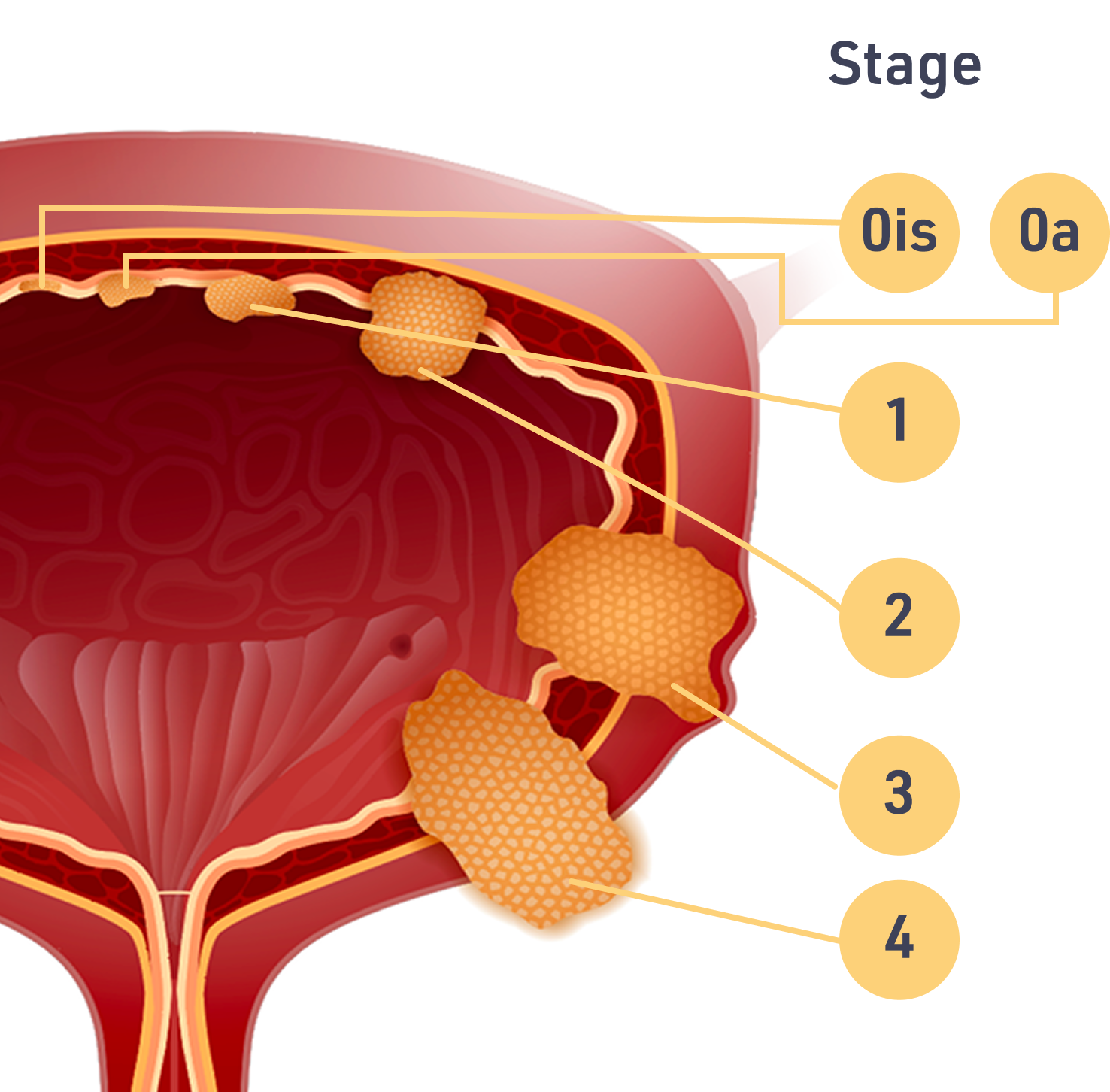
Staging Bladder Cancer
When doctors look at bladder cancer, they try to figure out how deep the cancer is and how far it has spread. This is called staging. The higher the stage, the further the tumor has grown through the layers of the bladder wall.
These are the stages doctors use:
Sometimes the stages appear with a T before the number. That T stands for tumor. With or without the T, the stages are the same.
Grading Bladder Cancer
Grade measures how aggressive the cancer is. Bladder cancers are graded by how the cancer cells look under a microscope and how much they are multiplying. There are 2 grades: slow growing (low-grade or LG) and fast growing (high-grade or HG).
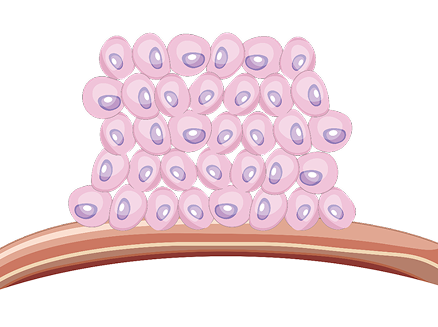
Normal cells
When normal cells reach a certain density, they stop dividing and enter a resting phase. This is not true of cancer cells.
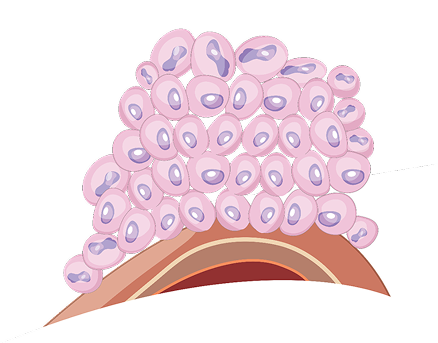
Slow growing (low-grade) cancer cells
These bladder cancer cells will likely grow and spread more slowly than fast-growing (high-grade) bladder cancer cells.
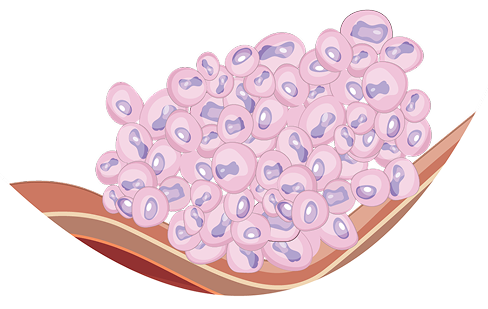
Fast growing (high-grade) cancer cells
These bladder cancer cells tend to be more aggressive. They are more likely to spread into the wall of the bladder and beyond. Most invasive bladder cancers are high-grade. They tend to be more difficult to treat.
The cancer's grade is separate from its stage. Ask your doctor to tell you the grade and stage of your tumor.
~55% of NMIBCs are low-grade (LG). This is the type of NMIBC this website focuses on.
Risk Levels
Treatment for NMIBC depends on how much risk there is of the cancer coming back after treatment, timing and frequency of recurrences (when the cancer comes back after it has been treated and thought to be gone), and the risk of spreading further (progression). The level of risk is determined based on several factors, including the stage, grade, size, and number of tumors that are present.
There are 3 risk levels: low risk, intermediate risk, and
high risk.There are many details that determine whether NMIBC is low risk, intermediate risk, or high risk. The table above gives you an idea of how complicated it can be.
For diagnosis, tumor samples will be removed and sent to a pathology lab for analysis. The pathology report will provide information such as the type, stage, and grade of cancer. Your doctor will use this report along with other factors to also determine your risk level.
If you do not know the grade or risk level of your cancer, ask your doctor. This is important information that will affect what kind of treatment you receive for your cancer.


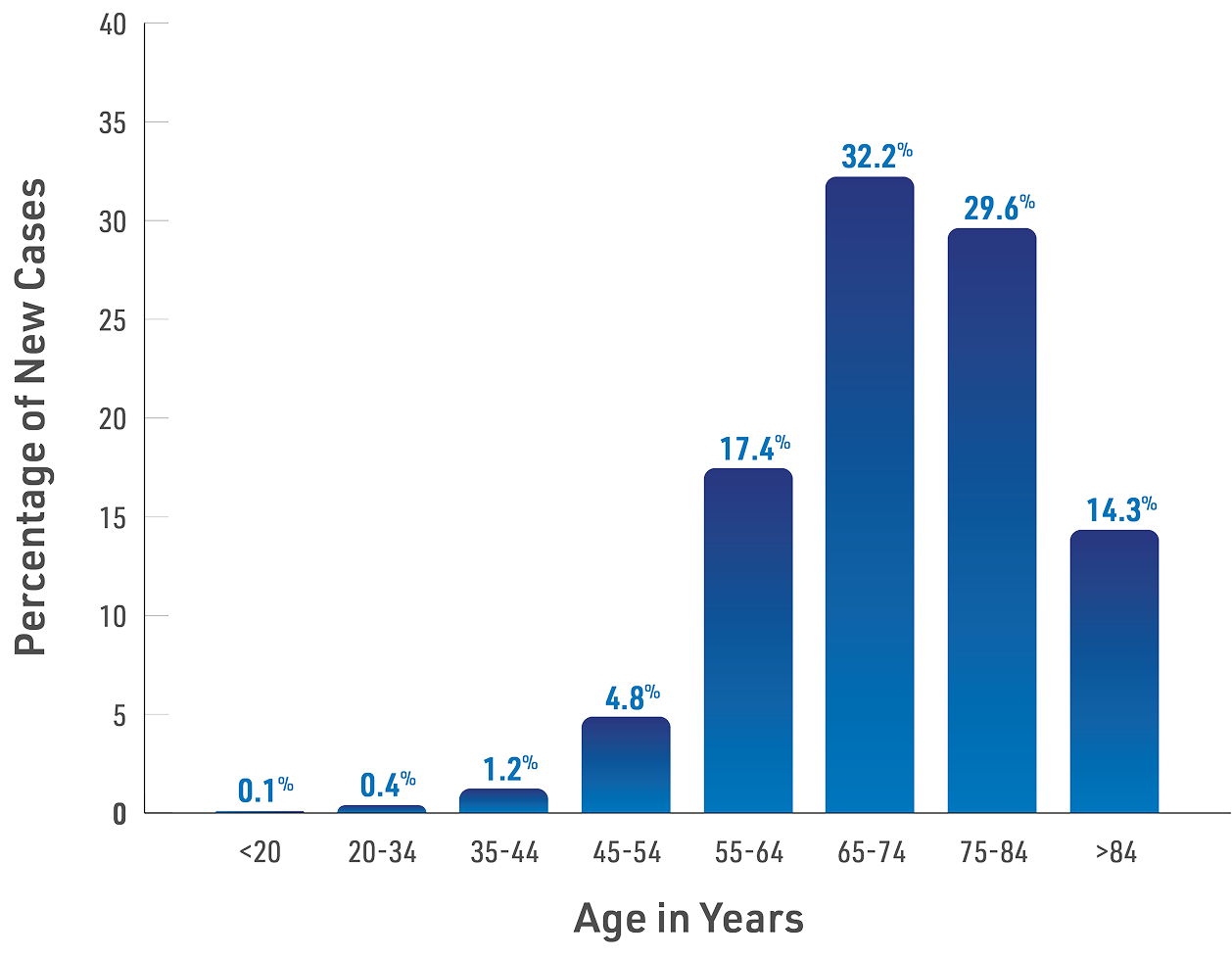
 Bladder cancer is most frequently diagnosed between ages 65 and 84, about 25% occurs in those <65 years old
Bladder cancer is most frequently diagnosed between ages 65 and 84, about 25% occurs in those <65 years old